 Mark Jennings
Mark Jennings Dr Nadeem Moghal
Dr Nadeem MoghalFrom our Founder
Foreword
Year after year the NHS sets out to move care closer to home, and year after year it drifts the other way. Every plan promises prevention and earlier treatment. Yet each year more of the work and more of the money ends up in the hospital. The ambition has never wavered; the delivery has never come.
The usual explanations are that people have not tried hard enough, or that the structures need another reorganisation. We think both miss the point. You cannot reorganise your way out of an incentive.
Instead, we ask why a system full of capable people, all wanting the same thing, keeps producing the opposite. The reason is structural. Money follows activity into the hospital, and so does clinical risk. At almost every level, the funded choice is to send the patient on. So is the safe one. No amount of effort overcomes a system tilted that way. The incentives themselves have to change.
What is new is that changing them is, at last, possible. Until recently, no one could route care across a whole population while holding the budget and the coordination in one place. Integrated Health Organisations (IHOs), set out in the 10 Year Health Plan, are the first credible vehicle for putting that capability to work. But the design has to be right. An Integrated Health Organisation built inside the hospital will, in the end, answer to the hospital. To reset the system, it has to sit across the whole of it, rather than inside the part that already dominates.
At Strasys we spend our days on this kind of problem: why health systems that want one thing keep doing another, and what it takes to change the decision rather than repeat the plea. This paper is our reading of the opportunity an IHO presents. Some of the detail will be wrong, and the design choices belong to others. We stand behind the central argument.
Get the design right, and the shift the NHS has chased for a generation stops being a slogan and becomes the way the system behaves by default. The pull that has defeated every previous attempt can be made to work in the patient’s favour. That is the prize, and for the first time it is within reach.

Naeem Younis
Founder and Chief Executive, Strasys
The paper is written by Mark Jennings and Dr Nadeem Moghal. It draws on the NHS 10 Year Health Plan, the Integrated Health Organisation model set out by the NHS Alliance, and our Decision Intelligence work with NHS leaders.
In short
The Argument in Brief
Every incentive pushes the wrong way
Cost and risk both travel up the stack, so the system drifts right while everyone agrees care should move left.
We have held the budget before, and it did not work
GP fundholding, PCTs, CCGs and ICBs all held a population budget. None reset the gradient.
What is different now is capability
Communications and AI make intelligent triage at population scale possible for the first time.
Organise around the job, not the silo
The system does six distinct jobs. Fund and run each on its own logic.
Begin with one move
One entity holds triage and a capitated budget for a population, then grows the rest from there.
Why now
The conditions for change
None held for any previous attempt to move NHS care left.
The policy has arrived
The 10 Year Health Plan (2025) puts IHOs at the centre and lets qualifying advanced foundation trusts hold a capitated, whole-population budget.
The model is defined
The NHS Alliance describes the IHO as a contract-plus-governance model with a capitated contract, sub-contracts and a collaboration mechanism.
The capability exists
For the first time, intelligent triage at population scale lets one entity hold the budget and route patients together.
Who should read this
What this means
ICB chairs and chief executives
The IHO does not replace you. You remain the strategic commissioner that can delegate a capitated budget to an IHO and hold it to account.
Foundation trust CEOs and boards
The plan envisages advanced foundation trusts holding the budget. This is where you weigh stepping into that role.
Medical and clinical directors
Routing carries clinical accountability. The paper sets out the indemnity and regulatory footing that makes triage at scale safe.
National and regional policymakers
How to turn the 10 Year Plan's intent into an operating model that actually moves care left.
What to do now
Four low-regret first moves
None of these requires a reorganisation, a merger or a new building.
Decide who holds triage
Name the single entity that holds triage and care coordination for your population.
Define the budget and its control
Set the capitated budget and the allocative control that comes with it.
Map the six jobs
Set out the six jobs to be done and how each is funded today.
Set accountability for routing
Establish the clinical, indemnity and regulatory footing for every routing decision.
If you only do one thing: put triage and the budget under one entity that sits across the whole gradient, and grow the rest from there.
The full paper
Read the complete argument
Introduction
Why IHOs sit at the centre of the 10 Year Plan, and the risk of defining one by its budget alone.
The incentive problem
Cost and risk both travel up the stack, so the system drifts right while care should move left.
Why this time is different
Fundholding, PCTs, CCGs and ICBs all held the budget. What is new now is the capability to route.
Six jobs to be done
The system does six distinct jobs. Fund and run each on its own logic, not in silos.
Where to begin
Begin with one move: one entity holds triage and a capitated budget for a population.
Owning triage
What it takes to hold routing at population scale, and the footing that makes it safe.
A commissioner with teeth
The allocative control an IHO needs to actually move care, not just review it.
Outcome follows incentive
Reset the gradient and the system stops drifting. Outcome follows incentive.
Introduction
Why IHOs, and why now
Integrated Health Organisations (IHOs) are central to the direction of travel in England’s health policy. The 10 Year Health Plan defines an IHO chiefly by its financial mechanism (a capitated whole-population budget), which may be held by qualifying advanced NHS foundation trusts.[1] The NHS Alliance has further defined IHOs as a contract-plus-governance model layered onto existing organisations, with a three-part structure comprising a capitated contract, sub-contracts, and a collaboration mechanism.[2] Within these definitions, the IHO risks becoming a label attached to existing structures rather than a fundamentally new organising idea. This would be a waste. Strasys regards IHOs as a huge opportunity to address structural deficiencies within the NHS. We further view IHOs as a viable way (the only one we see at present) to successfully deliver the left shifts from treatment to prevention and from hospital to community, enabled by analogue-to-digital shift. This paper explains why.
A clear intent runs through English health policy: to bring diagnosis and treatment closer to the patient’s first point of need, and increasingly ahead of it. This falls under the broad term ‘left shift’. The intent faces two primary obstacles to delivery. The first is that the system’s incentives push the other way; the second is that the capability to route care intelligently at a population scale has not previously existed. Patients have entered the system via primary care (GP) or A&E and then been routed via escalation up the stack of clinical specialties. Digital services and AI now provide radically different options for this second obstacle, the promise of accurately routing patients at scale directly to the optimal part of the system. The IHO should be the entity that addresses the first obstacle, the incentives pushing in the wrong direction, and thus turns a shared ambition into an operating reality.
The incentive problem
What the IHO has to address: the incentives all push the wrong way
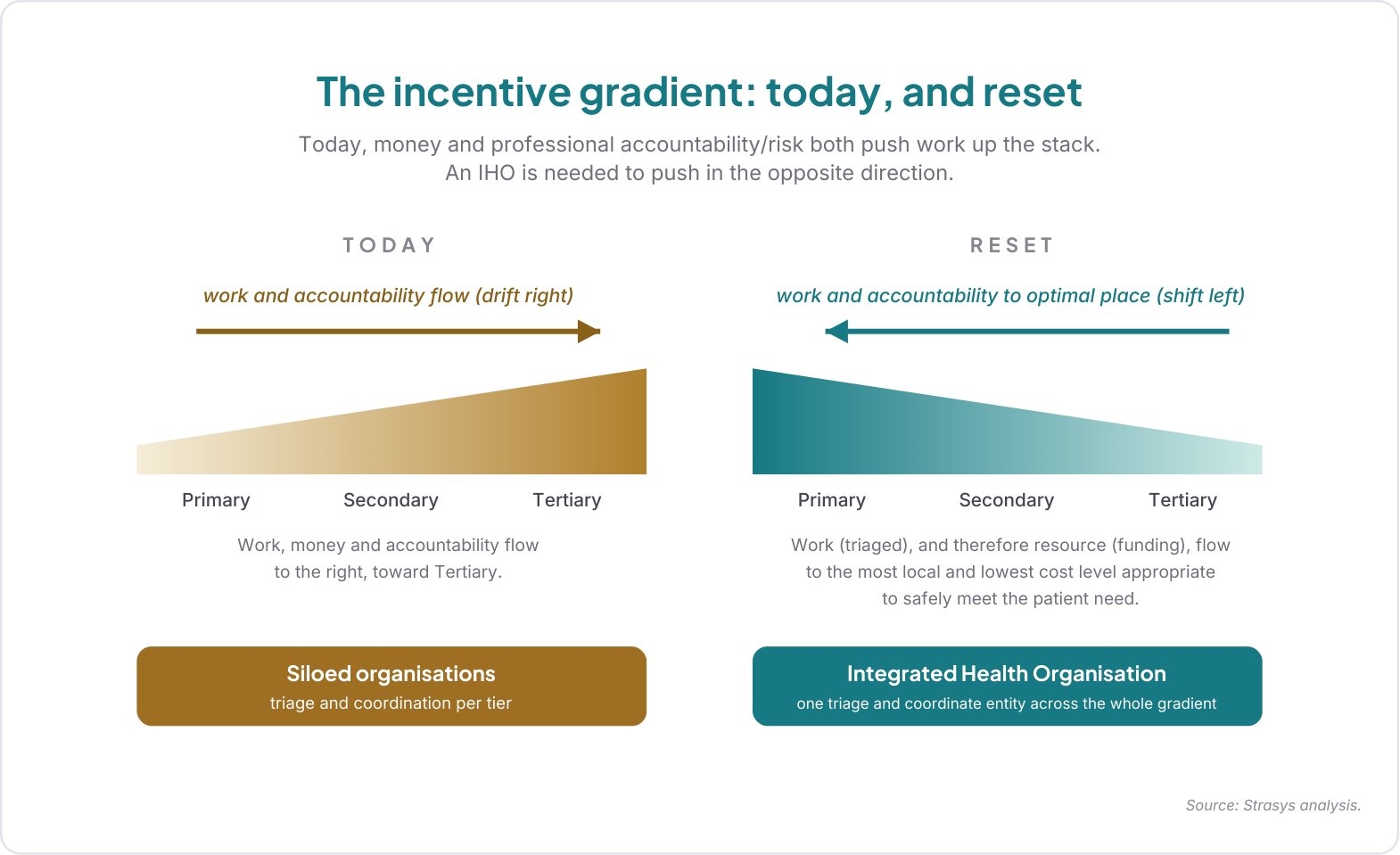
Almost everyone agrees on the need to move care closer to the patient: prevent more, diagnose earlier, treat at the lowest appropriate level. Yet the system drifts in the other direction, with more activity reclassified as complex and increasing pressure on the acute tier every year. Many individual clinicians and organisations make Herculean efforts to resist the drift to the right, but the pull is gravitational, and finding the incentives puts unnecessary stress on the system and the people within it.
The reason is that the incentives run the wrong way, to the right, not the left, and they do so twice over. The funding model incentivises throughput at the most complex and expensive end of the stack, where elective and specialist activity is paid per case, and is broadly indifferent to throughput at the lower-cost end, where primary care is capitated, and emergency and community work is largely block-funded. The professional risk runs the same way: a clinician earns no reward for making an early call and carrying the risk of being wrong but bears real consequences when a call proves incorrect; so, when in doubt, the safe move at every level is to defer the decision upward. Closely related to this, funding constraints deter test activity at each level, reinforcing a tendency to refer up for testing, guidance and diagnosis. Cost and risk both travel up the stack. The left shift asks people to move against the incentive gradient.
You cannot force a system to move against a gradient. Either the system, the gradient (incentives), or both need a reset for alignment. A gradient that runs between tiers cannot be reset by any actor sitting within a tier; it can only be changed by an entity that sits across the whole of it.
That entity is what an IHO should be.
Why this time is different
Why this differs from what we have tried before
England has created cross-tier, population-scale, capitated budget-holders before: GP fundholding, Primary Care Trusts, Accountable Care Organisations, Clinical Commissioning Groups, and today’s Integrated Care Boards. Each held a budget across a population, but none altered the incentive gradient. The case for the IHO has to explain why this time is different.
The difference is capability. Previous budget-holders could commission across the gradient, but they could not operate patient routing at scale, so they remained purchasers negotiating with providers who owned the patient relationship. Modern digital technologies, particularly in communications and AI, change that. Intelligent triage at scale is now possible for the first time, allowing a single entity to hold the budget and run routing together. The fusion of those two functions is what resets the gradient. Being able to direct both resource allocation and work allocation is essential to an effective IHO.
Six jobs to be done
What the IHO has to organise: six jobs to be done
To route care to the right place, the IHO needs to map the patient's needs to the relevant service provider for the job to be done. The traditional mapping (primary, secondary, tertiary, community, mental health) describes organisational siloes of service delivery, the distribution mechanism, rather than the product, i.e. the actual job to be done. The more useful mapping is directly to the job to be done, the product, because that determines how the service should be staffed, funded and evaluated.
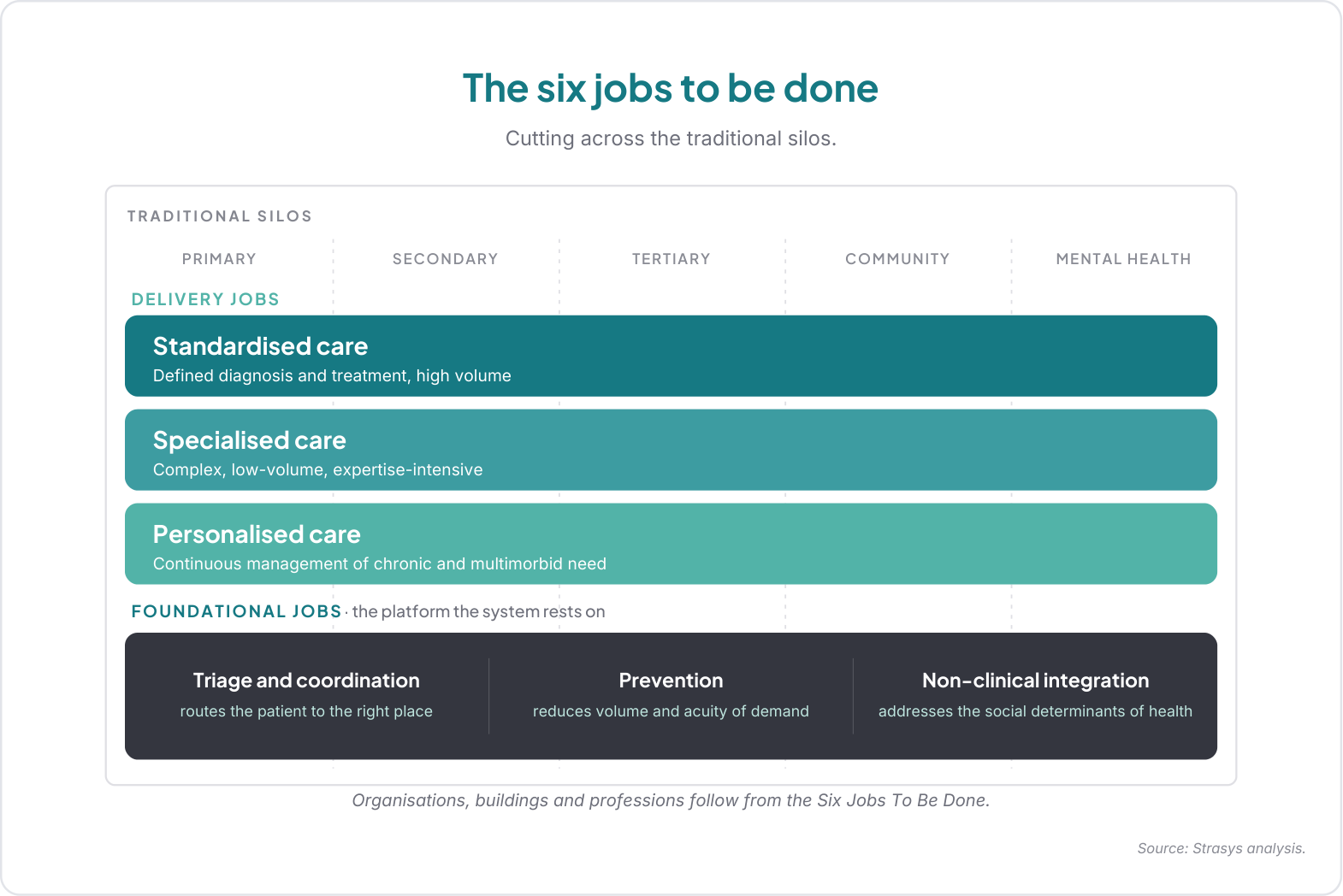
We propose a new lens, deliberately radical. It is built from the jobs to be done for patients: form follows function, product before distribution. On this view, the system delivers six distinct jobs that cut across the old silos.
- Three foundational jobs the whole system rests on: triage & coordination, prevention, and non-clinical integration (addressing the socio-economic drivers of demand).
- Three delivery jobs through which clinical care is provided: standardised care (well-defined diagnosis and treatment, high volume), specialised care (complex, low-volume, expertise-intensive), and personalised care (continuous management of chronic and multimorbid need).
The design principle is to modularise delivery and integrate coordination. Each delivery job has its own cost structure and definition of success, and each should be run as its own ‘business’, funded on its own logic. Today, they are conflated within single institutions, so simple work bears the cost and disruption of the most complex, and the foundational jobs that would reduce demand at the source are starved because no one is paid or structured to run them. Separating the delivery jobs entails some necessary handoffs, but we argue these will be fewer and easier than the current system’s, with correspondingly lower coordination costs. Within an IHO, the triage and coordination layer is what absorbs the handoffs: the same function that routes the patient also holds the pathway together across jobs, which matters most for the frail, multimorbid patient who needs several jobs to be either in parallel or sequence. The IHO is the entity that commissions and balances all six jobs across a population.
Triage and coordination
The connective layer that routes each patient and holds the pathway together across jobs.
Prevention
Keeping people well and reducing demand at the source.
Non-clinical integration
Acting on the socio-economic drivers of demand.
Standardised care
Well-defined diagnosis and treatment, high volume, delivered locally.
Specialised care
Complex, low-volume, expertise-intensive care, reached by disciplined triage.
Personalised care
Continuous management of chronic and multimorbid need.
Where to begin
The end-state is ambitious; the starting point is radical but simple
Taken to its conclusion, this is an ambitious end-state: dynamic allocation of funding, and therefore resources, matched to where patient need is best met within an end-to-end healthcare system organised around the jobs to be done for patients. It sounds idealistic, so credibility depends on a viable path from where we are today.
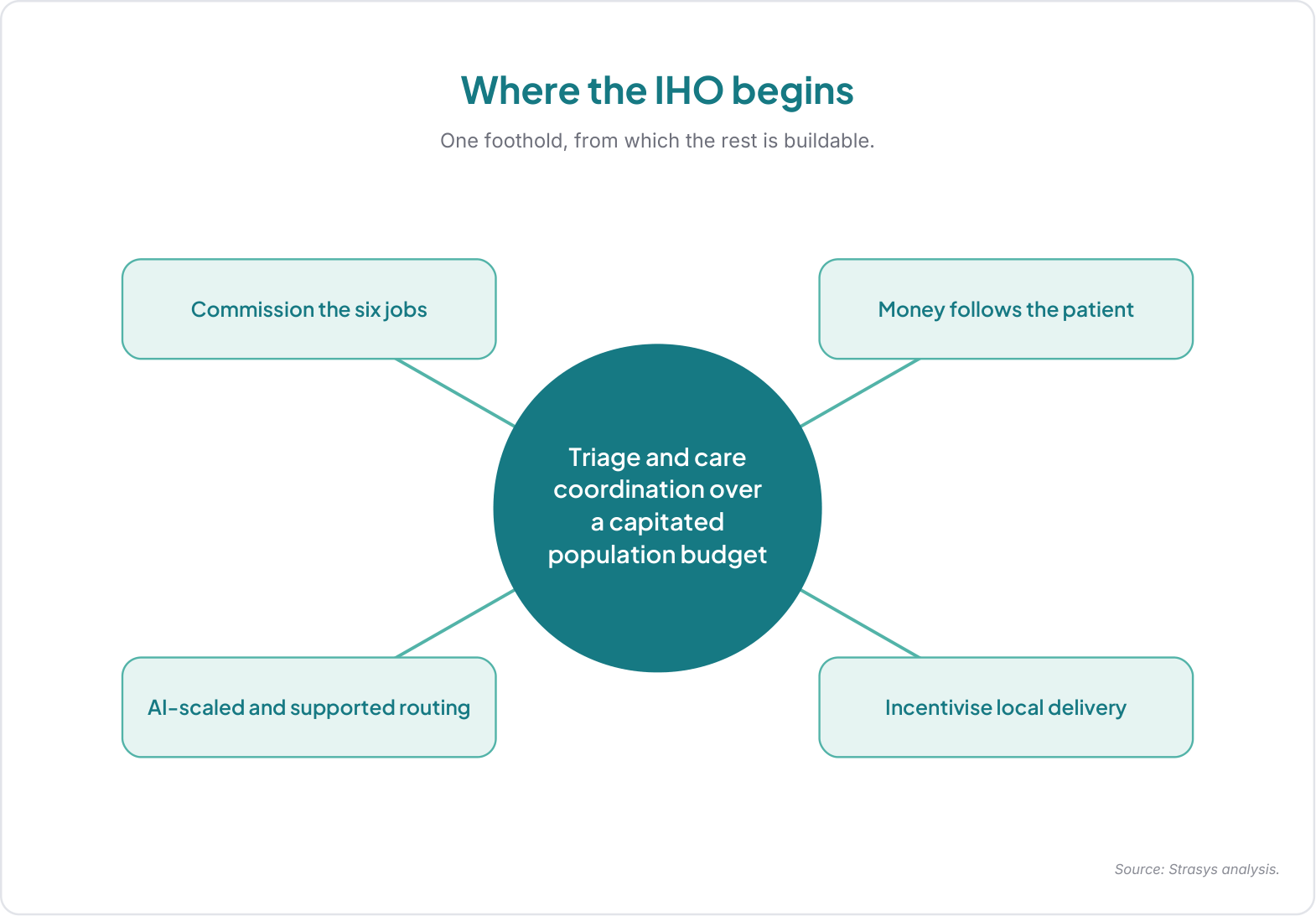
Where does an IHO begin? It begins with one thing:
An Integrated Health Organisation being the single entity that holds triage and care coordination for a defined population, and exercises allocative control over a capitated budget for that population.
IHOs do not inherently require reorganisations, mergers, or new buildings, but they do require significant digital, triage, and commissioning capabilities alongside ownership of a capitated budget. Triage and coordination give the IHO the means to decide where each patient should go, replacing the slow discovery of the right destination by failure to diagnose at each level. The capitated budget gives it the incentive to shift left and drive efficiency: when one entity holds the money for a population, keeping that population well and treating them at the lowest appropriate level becomes the whole point of the job. From that foothold, the IHO can commission the six jobs to be done, fund each on its own basis, and scale the triage as it proves itself. Begin with triage and the budget under one roof, and grow the rest from there.
Owning triage
What it means to own triage and care coordination
Routes into the existing NHS system almost always start with a physical presentation at a primary care centre or A&E. Some patients have previously contacted NHS 111 and had a conversation, scripted on the NHS end, that directed them to one of those physical presentation points. At presentation, the clinician may or may not have relevant medical records available, but in most cases, a history will be taken, tests may be performed or, more likely, requested, and the patient will then be directed through the system as appropriate. With handoffs between care organisations, there is a retake of the history, often a repeat of tests, followed by additional tests and evaluations as needed to reach a diagnosis and treatment plan. Sequential steps, duplications, and handoffs within the process drive delays and costs. In many cases, NHS England’s pathway already prescribes an IHO-shaped fix to more complex diagnostics. For example, unspecified breathlessness should be addressed through a “one-stop-shop” assessment at a community diagnostic centre and a multidisciplinary meeting for unspecified breathlessness, rather than sequential single-organ referrals. The Strasys vision of the IHO provides the incentive and routing ownership to consistently deliver what the pathway already recommends but is often impeded by today’s realities.
IHOs can only be transformative if the initial test and triage process is held by the IHO and abstracted from service delivery silos. Patients (or people acting on their behalf) contact digital services, with full access to relevant medical records, to articulate their symptoms or needs. Those digital services could range from standard AI chats to video consultations with emergency medics or even specialist teams for cases such as strokes, all accessed via a single digital front-door with telephony alternatives to support inclusion. From that initial contact, the patient can be brought in for immediate treatment, booked for tests prior to a consultation, or scheduled for an appointment with a clinician, appropriately prioritised for their history, need and acuity. In non-urgent cases, and where tests are needed to support a diagnosis based on the clinician’s assessment, they should be taken, with results available before the appointment.
All of this is possible with the services and technology available today. At the current exponential rate of AI improvement, the extent to which such a triage process can be supported by primarily automated probabilistic solutions that perform far beyond the capabilities of top human clinicians is increasing by the month. IHOs need to be envisaged for where capability is headed, not just where it is today.
Abstracting triage from points of service delivery means you can dramatically expand the range of those points. Facilities such as community diagnostic centres and neighbourhood treatment centres can be used for local testing, hot clinics, and for shifting a large proportion of current urgent and emergency care to a scheduled basis. The assets already exist, or are planned; this is just about how they can best be used. IHOs can drive up the volume of testing whilst driving down the marginal cost, sharing economies of scale across a large population base and supporting earlier diagnosis.
IHOs, rather than Primary Care, would own patients’ medical records and would be responsible for tracking the timely, safe and effective transition of each patient through the system. GPs primarily focus on the Personalisation job-to-be-done, supporting people with chronic conditions and ensuring continuity of care. They play an essential role in coordinating such care but no longer need to track the more transactional elements of care for Standardisation and Specialisation patients, e.g., whether the requisite tests or procedures have been done. Digital solutions at the IHO level track the many thousands of activities across patients in the system, with safety nets to ensure steps are not missed; they provide transactional integrity and continuity, whereas GPs provide the human element of continuity of care for those most in need.
A commissioner with teeth
A commissioner with teeth
To drive the necessary change within the NHS, all parts under the IHO should transition to activity-based payment models. The precise nature of these activity-based payment models would ideally vary based on the work to be done, i.e., standardisation jobs paid based on outputs to optimise efficiency, personalisation jobs paid on subscription or case-based capitation to incentivise proactivity, and specialisation jobs paid based on specialist benchmarks tied to case complexity and outcomes.
Owning both the triage (i.e. the allocation of work) and the funding (payment for that work) will give IHOs the real teeth necessary to commission work and be exacting in the standards to which that work is delivered.
Owning the patient relationship and the triage function is what gives the IHO teeth. Because it routes the patient, the IHO decides which provider sees them, and it can shift a component of a pathway from one provider to another. The provider that keeps people well and treats them at the right level wins the work; the provider that does not, loses it. That is how the motive at the top of the system transmits into changed behaviour across it.
Two things must be true for this to hold. First, the IHO needs real reach over how providers are engaged and paid for components of services. Much of that reach is bounded today by nationally set contracts and tariffs, so the IHO’s allocative control begins inside the envelope those allow and widens as national arrangements adapt to support it. An IHO with genuine teeth threatens provider income by design and will be resisted, so its authority to reallocate work has to be explicit and backed, or the interests it exists to redirect will mute its effectiveness. This reach is a precondition that the IHO builds toward over time, and it does not necessarily hold from day one. Dynamic allocation of funding (money follows activity) obviously needs to be balanced with the necessary stability of income for resourcing and capital investment, but the proposed model ensures long-term activity shifts within the system are matched by funding shifts.
Second, resetting the money gradient leaves the risk gradient in place unless accountability moves with the routing. A triage function that routes a patient to a lower tier must own that decision, with clinical accountability, indemnity, and a regulatory footing that treats any routing decision (human, AI, or hybrid) as a defensible standard of care. Absent that, the old caution returns at the new triage layer, clinicians escalate to be safe, and the system rebuilds triage-by-failure inside the IHO. The capitated budget answers the money; clear accountability for routing answers the risk. The IHO needs both.
Outcome follows incentive
Outcome follows incentive
Defined this way, the IHO is the vehicle that finally delivers the shared intent for care closer to, or ahead of, each patient’s point of need. The left shift becomes the natural consequence of a reversed gradient for aligned incentives. Neighbourhood health becomes where most personalised and standardised care is delivered. Prevention becomes fundable, because a single entity holds the population budget that gains from it. Digital services and AI support the triage and coordination engine that makes routing at population scale possible. Outcome follows incentive: put triage and a capitated budget for a population under one entity that sits across the full gradient, give it the teeth to act on what the triage tells it, and the rest follows.
A positive vision for the future of UK healthcare depends on recognising and starting with patient need, and addressing the jobs to be done in a way that aligns incentives in the right direction for both efficiency and safe, high-quality care. By Thinking Differently, Strasys have a unique perspective on IHOs as the keystone for an NHS fit for its second century.
From idea to action
An IHO board briefing for your system
The hard part is not the idea, it is the first move in your own system. We can prepare a short board briefing that applies this thinking to your population. It is grounded in your context, not a generic template.
- Where an IHO would begin for your population
- The triage, digital and commissioning capability you already hold
- The capitated budget and allocative control you would need
- The accountability and regulatory footing for routing
- The first decisions for your board, including the cost of doing nothing
This is what Decision Intelligence for healthcare means in practice. Not another strategy, but a clearer decision.
Request a board briefingRelevant Strasys capabilities
Routing at population scale is a Decision Intelligence problem. The same thinking runs through our work on board capability, clinical service redesign, value and workforce.
Questions about IHOs
Take it to your board
Get the full article
Add your details and download the complete Point of View to read and share with your board.
Thank you. The full article is opening now.
References
- Department of Health and Social Care (2025). Fit for the future: 10 Year Health Plan for England. CP 1350. London. gov.uk
- NHS Confederation (2025), now the NHS Alliance. Towards integrated health organisations: considerations for policy and NHS leaders. London. nhsconfed.org